 Issue PDF
Issue PDFHandoffs
Handoffs, in the most concise description, are an exchange of responsibility for one or more patients from one provider to another. Handoffs are “conversations rather than reports”1 and typically consist of four phases—preparation (by both parties), patient arrival in the new location, the actual handoff (e.g., RN-MD interaction), and post-handoff management by the receiving clinician.2 The practice of perioperative care involves frequent transitions of patients between multiple providers and areas of care. Well-conducted handoffs are critical for information exchange that enables relieving clinicians to provide care with the same factual and tacit knowledge of the patient as each and every previous provider. A handoff is an opportunity to review care and potentially correct mistakes; however, poor handoffs may lead to information loss and adverse patient outcomes.3–5 Some of the major contributors to poor handoffs include distractions, interruptions, inadequate preparation, lack of a structured report, lack of understanding, production pressure, incomplete information exchange, and poor interpersonal interactions. The interactions between anesthesia providers and other medical professionals can be a source of a significant portion of all handoffs for a patient during their hospital course. This article will discuss the main perioperative transitions of care (Figure 1) and how they differ.
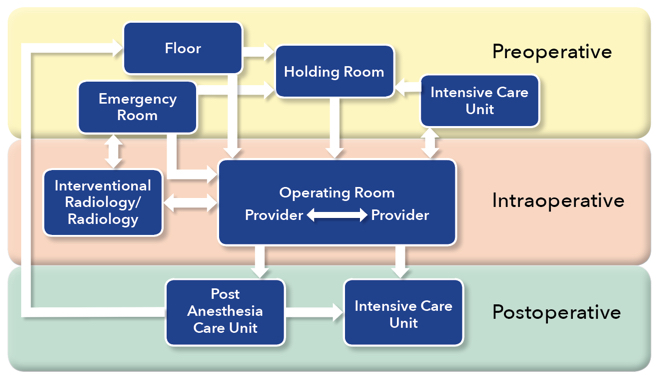
Figure 1. Perioperative Handoffs. Each arrow indicates a handoff.
Preoperative
Holding Room (Area) to Operating Room
Most patients begin their operative course in a holding room, where they typically encounter pre-operative nursing, anesthesia providers, and their surgical team. The preoperative handoff thus begins in the holding room; yet little information exists on these preoperative interactions. Holding room handoffs usually involve information transfer between the patient or family member, a holding room nurse, an operating room (OR) nurse, an anesthesia team member, and may or may not include a surgical team member. The quality and content of the information communicated varies significantly.
Seven percent of anesthesia-related post anesthesia care unit (PACU) closed claims were related to preoperative preparation, and communication issues were classified as a contributing factor in 14% of the 419 recovery room incidents.4 The authors suggested that improvements in written, verbal, and electronic transmission of information should be addressed. A pediatric preoperative handoff study implemented a preoperative checklist that was associated with an improvement in 12 of 15 key items being discussed among providers.6
Floor/Emergency Room/Intensive Care Unit to Operating Room
Patients do not always arrive to the OR from a holding room. They may come to the OR from any number of locations, such as the emergency department, a medical/surgical floor, or the intensive care unit (ICU), either directly or via the holding room. The variability in culture in these locations presents its own challenges and barriers, as each location may have different preparation techniques prior to OR transfer. Team composition, policies, charting, and methods of communication may differ from unit to unit. In addition, there may be limited information available due to the emergent nature of some procedures. In a study of neonatal intensive care unit (NICU) to OR handoffs, several barriers to information exchange were discovered.7 These included lack of a standardized report, lack of patient preparation for transfer, unclear transition of care between team members, unclear provider roles, significant provider traffic in and out of the room, and distractions or interruptions. Not only do the providers present at the time of handoff vary widely, but up to 10 different providers were present at any given handoff. In addition, the perception of handoff quality varied widely between NICU providers (MDs, RNs, NPs) and anesthesia providers (MDs, CRNAs, RNs), with 41% reporting “fair” to “poor” and only 35% reporting “very good” to “excellent.” Caruso and colleagues suggested that standardizing ICU to OR handoffs increased communication without delaying surgery and improved anesthesia provider satisfaction scores.8
A study by Nagpal that followed 20 patients from the ward through their surgical course, found that the preprocedural teamwork phase had the largest number of failures (61.7%).9 Although the anesthesia team had 86.6% of necessary preoperative information and the surgical team had 82.9% of necessary information, the nursing team only had 25% of the total information and only 27% of the total information was known by all primary team members (surgeon, anesthesia provider, surgical assistant, scrub technician, and circulating nurse). Verbal handoff from the ward to the OR team only occurred in 43% of the patients, and in 10% of the cases there was no communication between the ward nurse and the OR team receiving the patient. The study reported that information transfer failures contributed to a total of 18 incidents and adverse events in 15 of the 20 patients. In another study by Nagpal, three types of information transfer and communication failures were described in the preoperative phase: source failures (information in different places, consents missing, inadequate documentation), transmission failures (lack of communication between anesthesia and surgical teams, lack of communication between the ward and OR staff, information not relayed), and receiver failures (specialists’ opinions not followed, checklists not followed).10 These failures had adverse effects on patients, teams, and the organization (such as case cancellations, increased provider stress, and wastage of resources), but these effects were not linked to any particular phase of failure.10
Intraoperative
Provider to Provider
To our knowledge, only a handful of studies exist on intraoperative handoffs. Handoffs between anesthesia providers may be for short-duty relief breaks or shift-to-shift relief. However, their presence may be associated with quantifiably increased morbidity and mortality,11 and the association appears to be strengthened with each additional handoff. On the other hand, there may be a benefit associated with intraoperative handoffs, in that they may bring a fresh set of eyes to discover issues and errors.3
The intraoperative period must be considered a part of the transition from preoperative to postoperative care, and handoffs within that setting should be treated similarly. However, the intraoperative handoff is often rushed, conversational, and not well-structured. The entirety of the perioperative course may benefit from improved, structured communication,12 and the intraoperative course is no exception. The quality of intraoperative handoffs has substantial variability,13 depending on location, setting, and culture. Structured handoffs in a pediatric population have have been shown to result in decreased communication errors and increased reliability and effectiveness of communication in the operating room.14 Agarwala performed a study showing that an electronic checklist improved relay and retention of critical information at intraoperative handoff of care.15
Location/Procedure Change
Some situations require a change in location and staff due to surgical issues or needs. For example, some institutions provide different anesthetics for multiple procedures at multiple locations on a single infant or child to minimize the number of exposures to general anesthesia.16 At other times, patients may require additional testing during an anesthetic such as interventional or radiological imaging as part of a surgical procedure. In addition, a second operative team may take part in the procedure, and their presence at the initial handoff or time-out is unlikely to be consistent.
These changes in procedure and location lead to multiple handoffs between anesthesia, surgical, nursing, and technical staff, and often require additional team members who may not have been part of the initial preoperative handoff and, therefore, will likely have limited information regarding the patient. These handoffs inevitably add complexity to the procedural care of the patient. Strategies to manage the increased complexity include adding an additional time-out when a new team assumes care of the patient, recounting instruments and supplies, and mandatory surgical site imaging post-procedure. Regardless of the strategy, providers must recognize these changes as handoffs of care.
Postoperative
Operating Room to Post Anesthesia Care Unit (PACU)
Postoperative handoffs are the most common and well-studied handoffs in the field of anesthesiology. These typically involve anesthesia staff reporting to PACU nursing staff and may also involve surgical team members. In studies of routine postoperative handoffs, it was found that significant amounts of information were frequently missed, such as ASA status, antibiotics received, and fluid administration.17 Handoffs of ambulatory patients also commonly resulted in omission of data and resulted in poor receiver satisfaction.18 Composites of overall handoff quality are judged to be “good” less than half of the time following patient delivery to the PACU,19 and the variable quality of communication of pertinent case events in most postoperative handoffs is associated with a perceived increase in complication rates.13,20 As for claims data, 14% of anesthesia-related PACU issues were attributed to failures or deficiencies in communication.4
As noted above, structured handoffs in a pediatric population have been shown to significantly decrease communication errors and increase reliability and effectiveness of communication in the OR, and also in the PACU.14 Nagpal also reported a decrease in information omission and task errors and an increase in staff satisfaction after institution of a standardized handoff tool.12 Another study showed that a multimodal intervention substantially improved PACU handoffs, and the effect continued to be present 3 years after the intervention.21 Overall, the data available supports the use of a structured approach to postoperative handoff that includes a tool and education about its use.
Operating Room to Intensive Care Unit (ICU)
OR to ICU handoffs often include anesthesiology and surgical team members, OR nursing, and ICU team members, which may include physicians, nurse practitioners, physician assistants, nursing staff, respiratory therapists, and others. In some cases, the handoff from the operating room to the ICU may be the first structured handoff in a patient’s hospital course, especially in emergency situations. Although many of these studies have limitations, standardized ICU handoffs may be associated with reduced long-term ICU complications.22
Improvement in the safety and quality of handoffs of patients from surgery to the ICU may occur through the adoption of the Formula 1 pit stop/aviation structured approaches.23 Zoccoli et al. also reported the perception of improved consistency of data shared during handoffs and an increase in interdisciplinary communication by nursing staff following institution of a standardized handoff tool in the surgical intensive care unit.24 Many studies have examined OR to ICU handoff processes in the cardiovascular ICU. However, it is clear that other care environments require further studies to clarify the optimal way to perform a patient handoff.
Summary
While much of the data regarding handoffs and outcomes has been generated from postoperative and a few intraoperative exchanges, many of the barriers to effective communication exchange are universal, such as patient complexity, distractions, provider fatigue, time constraints, multi-tasking, and situational awareness/appreciation for different roles.25 Additional work in this area would likely improve understanding of these deficits and improve patient safety and provider satisfaction.
Dr. Lorinc is an Assistant Professor in the Division of Pediatric Anesthesiology at Monroe Carell Jr. Children’s Hospital at Vanderbilt University Medical Center in Nashville, TN.
Dr. Henson is an Assistant Professor in the Department of Anesthesiology/Division of Critical Care Anesthesiology at Vanderbilt University Medical Center in Nashville, TN.
Neither of the authors report any conflicts of interest to disclose pertaining to this article.
References
- Brandwijk M, Nemeth C, O’Connor M, et al. Distributed cognition: ICU handoffs conform to Grice’s Maxims. Chicago, IL: University of Chicago Cognitive Technologies Laboratory; 2003.
- Wears RL, Perry SJ, Eisenberg E, et al. Transitions in care: signovers in the emergency department. Proceedings of the Human Factors and Ergonomics Society Annual Meeting 2004;48:1625–28.
- Cooper JB, Long, DC, Newbower RS, et al. Critical incidents associated with intraoperative exchanges of anesthesia personnel. Anesthesiology 1982;56:456–61.
- Kluger MT, Bullock MFM. Recovery room incidents: a review of 419 reports from the Anaesthetic Incident Monitoring Study (AIMS). Anaesthesia 2002;57:1060–1066.
- Arora VM, Johnson JK, Meltzer DO, et al. A theoretical framework and competency-based approach to improving handoffs. Qual Saf Health Care 2008;17:11–4.
- Lorinc A, Crotts C, Sullivan M, et al. Pediatric preoperative handovers: does a checklist improve information exchange? ASA Abstracts 2016:1–2.
- Lorinc A, Roberts D, Slagle J, et al. Barriers to effective preoperative handover communication. Proceedings of the Human Factors and Ergonomics Society Annual Meeting 2014;58:1285–1298.
- Caruso TJ, Marquez JL, Gipp MS, et al. Standardized ICU to OR handoff increases communication without delaying surgery. Int J Health Care Qual Assur 2017;30:304–11.
- Nagpal K, Vats A, Wong H, et al. An evaluation of information transfer through the continuum of surgical care. Ann Surg 2010; 252:402–7.
- Nagpal K, Arora S, Vats A, et al. Failures in communication and information transfer across the surgical care pathway: interview study. BMJ Qual Saf 2012;21:843–9.
- Saager L, Hesler BD, You J, et al. Intraoperative transitions of anesthesia care and postoperative adverse outcomes. Anesthesiology 2014;121:695–706.
- Nagpal K, Abboudi M, Manchanda C, et al. Improving postoperative handover: a prospective observational study. Am J Surg 2013;206:494–501.
- Choromanski DW, Frederick J, Fattouch P, et al. Intraoperative hand over of patient information between anesthesia providers. Are we as good as we think we are? ASA Abstracts 2013:1–2.
- Boat AC, Spaeth JP. Handoff checklists improve the reliability of patient handoffs in the operating room and postanesthesia care unit. Kurth D, ed. Pediatr Anesth 2013;23:647–54.
- Agarwala AS, Firth PG, Albrecht MA, et al. An electronic checklist improves transfer and retention of critical information at intraoperative handoff of care. Anesth Analg 2015;120:96–104.
- Kilkelly J, Kinch J. An innovative paradigm: coordinating anesthetic care for complex pediatric patients requiring multiple procedures. J Anesth Clin Res 2015;5:490.
- Milby A, Böhmer A, Gerbershagen MU, et al. Quality of post-operative patient handover in the post-anaesthesia care unit: a prospective analysis. Acta Anaesthesiol Scand 2014;58:192–7.
- Pukenas EW, Deal ER, Allen E, et al. The ambulatory handoff: Fast-paced, high-stakes patient care transitions. ASA Abstracts 2014:1–2.
- Anwari JS. Quality of handover to the postanaesthesia care unit nurse. Anaesthesia 2002;57:484–500.
- Jayaswal S, Berry L, Leopold R, et al. Evaluating safety of handoffs between anesthesia care providers. Ochsner J 2011;11:99–101.
- Weinger MB, Slagle JM, Kuntz A, et al. A multimodal intervention improves postanesthesia care unit handovers. Anesth Analg 2015;121:95–71.
- Kaufmnan J, Twite M, Barrett C, et al. A handoff protocol from the cardiovascular operating room to cardiac ICU is associated with improvements in care beyond the immediate postoperative period. Jt Comm J Qual Patient Safety 2013;39:306–311.
- Catchpole KR, De Leval MR, McEwan A, et al. Patient handover from surgery to intensive care: using Formula 1 pit-stop and aviation models to improve safety and quality. Pediatric Anesthesia 2007;17:470–78.
- Zoccoli M, Castillo D. Improving continuity of patient care through the use of a universal handoff tool. ASA Abstracts 2014:1–2.
- Lane-Fall MB, Brooks AK, Wilkins SA, et al. Addressing the mandate for hand-off education: A focused review and recommendations for anesthesia resident curriculum development and evaluation. Anesthesiology 2014;120:218–229.