 Issue PDF
Issue PDFThe elimination of AKI after elective TJA, is possible. An anesthesiologist-led PSH initiative has resulted in a sustained reduction of a significant postoperative complication.
 The American Society of Anesthesiologists (ASA) defines a perioperative surgical home (PSH) as “a team-based model of care created by leaders within the ASA to help meet the demands of a rapidly approaching health care paradigm that will emphasize gratified providers, improved population health, reduced care costs and satisfied patients.” The PSH model of care was used by a team at St. Luke’ s University Health Network to reduce the incidence of Acute Kidney Injury (AKI) after elective total joint arthroplasty (TJA).
The American Society of Anesthesiologists (ASA) defines a perioperative surgical home (PSH) as “a team-based model of care created by leaders within the ASA to help meet the demands of a rapidly approaching health care paradigm that will emphasize gratified providers, improved population health, reduced care costs and satisfied patients.” The PSH model of care was used by a team at St. Luke’ s University Health Network to reduce the incidence of Acute Kidney Injury (AKI) after elective total joint arthroplasty (TJA).
AKI is a known complication after total joint arthroplasty. Rates reported in the literature vary from 2 to 15% for elective cases.1 The incidence of AKI may be underreported due to several factors. The absence of a creatinine measurement on postoperative day one, inconsistency in measuring urine output postoperatively, lack of recognition of AKI based on KDIGO criteria,2,3 and institutional differences in coding may all contribute to underreporting. An episode of AKI postoperatively may have negative short and long-term implications for patients4 and increased costs to the health care system.5,6
In 2016, a PSH-led initiative to reduce hypotension and AKI in our elective TJA population was initiated. A multidisciplinary team of anesthesia professionals, nephrologists, orthopedic surgeons, internal medicine hospitalists, nurses, EPIC analysts and a quality resource specialist was assembled. A protocol was developed and implemented with the following elements (Table 1):
- Screening of patients through our SOC (Surgical Optimization Center)
- Medication adjustment (ACE/ARBs/NSAIDs, diuretics) and standardized perioperative fluid replacement
- Standardized anesthetic management via ERAS protocol
- Withholding antihypertensive medications if systolic BP < 130
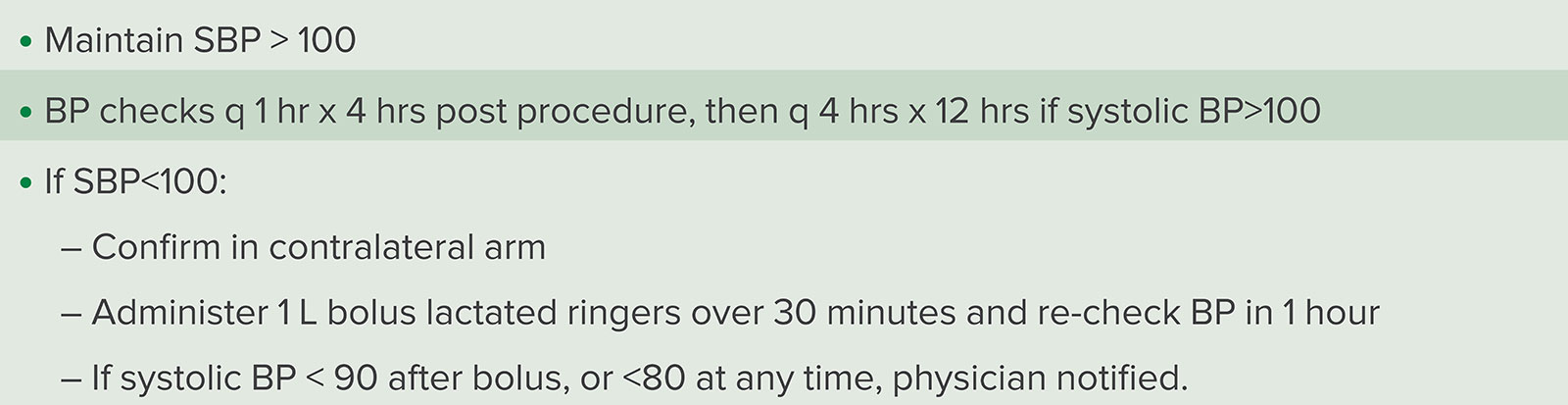
- Implementation of nursing-driven fluid protocol to allow postoperative treatment of hypotension (Table 2)
Table 1: Surgical Optimization Center AKI Risk Evaluation
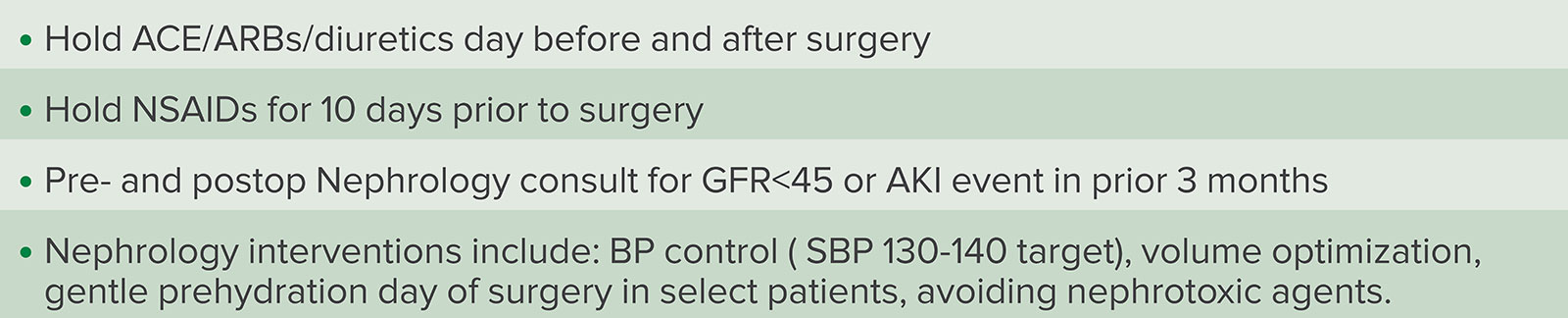
Table 2: Summary of Nursing Postop Hypotension Protocol
All patients undergoing TJA were included (Table 3). There were no exemptions for patients with pre-existing renal disease or revision surgery. Hypotension decreased from 12.7% to 5.9% and AKI from 6.2% to 1.2%. Further details of our PSH initiative were published in The Journal of Arthroplasty in June, 2018.7
Table 3: Patient Characteristics for the Perioperative Surgical Home Initiative to Reduce the Incidence of Acute Kidney Injury after Total Joint Arthroplasty

Since this publication, further enhancements were made to the protocol. They included:
- Increased preoperative focus on high-risk patients with preoperative nephrology consultation for patients with GFR < 45 mL/min and addition of gentle preprocedure intravenous hydration where indicated
- Addition of continuous postoperative vital signs monitoring including continuous pulse oximetry and automated vital signs gathering and real-time input into Electronic Medical Record (EMR) using Masimo Root and Patient SafetyNet Technology, (Irvine, CA).
- Further leveraging of EMR to improve protocol compliance, as well as rates of early detection of significant vital signs abnormalities (i.e., use of “smart alerts,” improved resolution of early-warning scoring systems via updating of EMR with continuous, real time vital sign monitoring)
After demonstrating success and sustainability at a single site, the protocol was expanded to additional network hospitals performing TJA. This included 21 additional surgeons performing procedures at nine hospitals. After network expansion, similar reductions in perioperative AKI from baseline were observed (5.9% to 0.6%) (Figure 1).
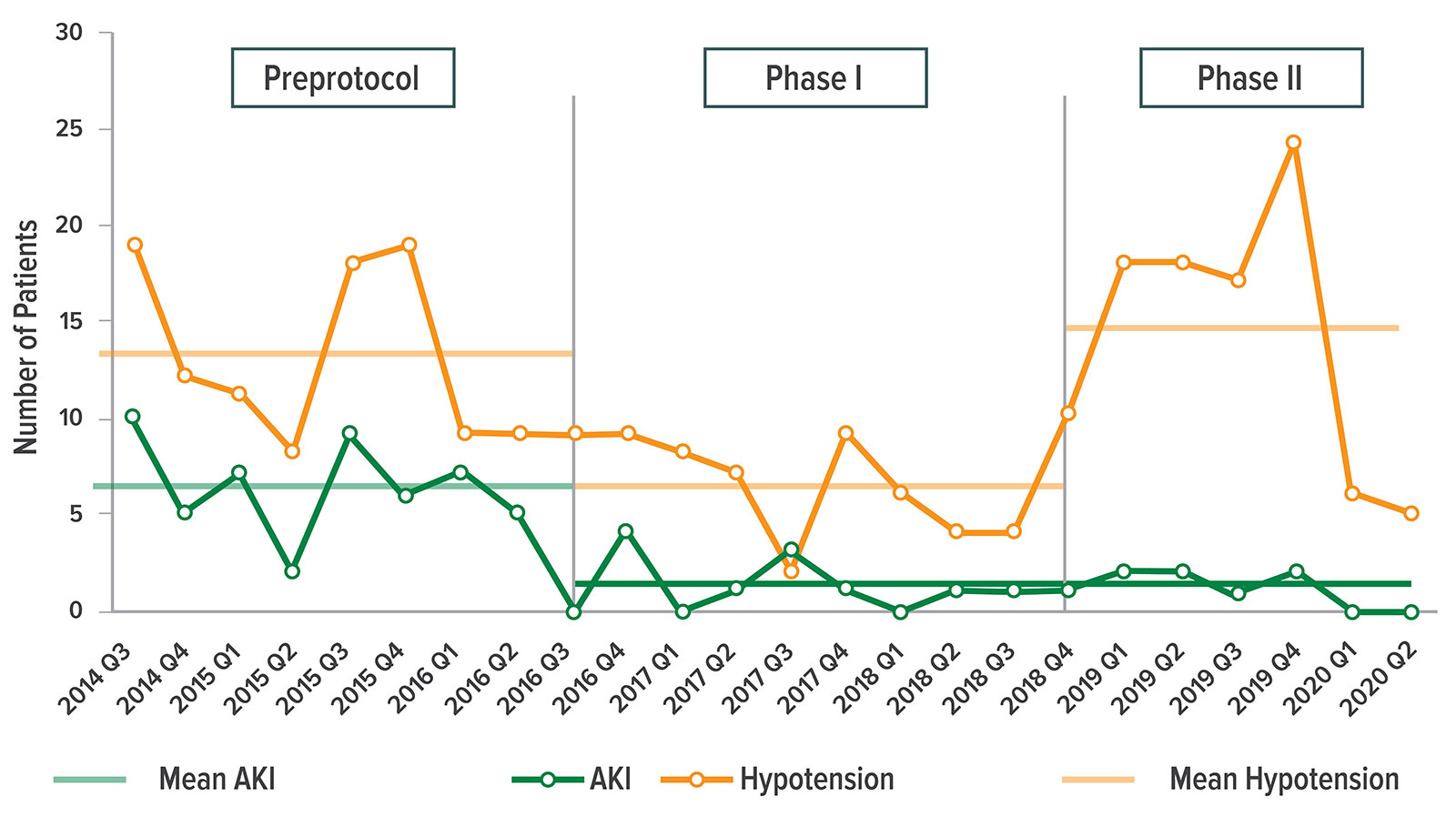
Figure 1: Changes in the frequency of perioperative hypotension and AKI before and during the 2 phases of the PSH initiative.
Overall, length of stay during this time period decreased from 2.75 days to 2.12 days (p< 0.01). Mortality rate was unchanged and 30-day readmissions were reduced from 3.8–3.2%, a trend which did not reach statistical significance.
At our University Hospital, based on KDIGO criteria, we have had a single case of AKI since November 2018 in 1,210 consecutive procedures ( primary, revision, or previous renal disease all included) at the time of this publication.
In summary, a multidisciplinary approach in the PSH model has led to sustained reductions of a significant complication following an elective surgical procedure. It has also raised awareness to the value of enhanced vital sign monitoring and avoidance of hypotension in the perioperative setting. A growing body of evidence suggests that perioperative hypotension is both common and underdiagnosed. Post-operative AKI may be a marker of global hypoperfusion, and cardiac troponin elevations in TJA patients have also been reported.8 Furthermore, hypotension is an important risk factor for perioperative myocardial injury after noncardiac surgery, which has been associated with worse perioperative outcomes.9 It is plausible that further improvement to patient care can be realized by expansion of real-time vital signs monitoring to other patient populations at increased risk for perioperative hypotension and AKI.10,11 Finally, although initiated by anesthesia professionals, the collaborative and multidisciplinary nature of this project was critical to its success. These outcomes could not have been achieved or sustained without our physician and nonphysician colleagues’ input and collaboration. This is a hallmark of a mature Perioperative Surgical Home and a model for future patient improvement projects.
Aldo Carmona, MD, is chief of Anesthesiology and senior VP of Clinical Integration at St. Luke’s University Hospital, Bethlehem, PA.
Christopher Roscher, MD, is section chief of Cardio-Thoracic Anesthesia at St. Luke’s University Hospital, Bethlehem, PA.
Daniel Herman, MD, is director of Perioperative Medicine at St. Luke’ s University Hospital, Bethlehem, PA.
Robert Gayner, MD, is chief of Nephrology and vice-president of Medical and Academic Affairs at St. Luke’ s University Hospital, Bethlehem, PA.
Ajith Malige, MD, is a PGY-V resident in the Department of Orthopedics at St. Luke’s University Hospital, Bethlehem, PA.
Brian Banas is a medical student at Geisinger Commonwealth School of Medicine,Scranton, PA.
The authors have no conflicts of interest.
References
- Kimmel LA, Wilson S, Janardan JD, et al. Incidence of acute kidney injury following total joint arthroplasty: a retrospective review by RIFLE criteria. Clin Kidney J. 2014;7:546–551.
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group: KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;1:le138.
- Luo X, Jiang L, Du B, et al. A comparison of different diagnostic criteria of acute kidney injury in critically ill patients. Crit Care. 2014;18:R144.
- Coca SG, Yusuf B, Shlipak MG, et al. Long-term risk of mortality and other adverse outcomes after acute kidney injury: a systemic review and meta-analysis. Am J Kidney Dis. 2009;53:961–973.
- Che1tow GM, Burdick E, Honour M, Bonventre N, Bates DW. Acute kidney injury, mortality, length of stay and costs in hospitalized patients. JAM Soc Nephrol. 2005;16:336570.
- Silver SA, Chertow GM. The economic consequences of acute kidney injury. Nephron. 2017;137:297-301.
- Lands VW, Malige A, Carmona A, et al. Reducing hypotension and acute kidney injury in the elective total joint arthroplasty population: a multi-disciplinary approach. J Arthroplasty. 2018;33:1686–1692.
- Bass AR, Rodriquez T, Hyun G, et al. Myocardial ischemia after hip and knee arthroplasty: incidence and risk factors. Int Orthop. 2015;39:2011–2016.
- Sessler D, Khanna A. Perioperative myocardial injury and the contribution of hypotension. Intens Care Med. 20l8;44:811–822.
- Futier E, Lefrant JY, Guinot PG, et al. Effect of individualized vs. standard blood pressure management strategies on postoperative organ dysfunction among high-risk patients undergoing major surgery: a randomized clinical trial. JAMA. 2017;318:1346–1357.
- Wu X, Jian Z, Ying J, et al. Optimal blood pressure decreases acute kidney injury after gastrointestinal surgery in elderly hypertensive patients: a randomized study: optimal blood pressure reduces acute kidney injury. J Clin Anesth. 2017;43:77–83.